05122542104, 9839088890
admin@kanpururologist.com
Urethra is a tube that carries urine out of bladder. Narrowing or blockage of this tube is known as stricture urethra. This disease is more common in men than in females.
Stricture can result from various causes:
The most common presenting symptoms are
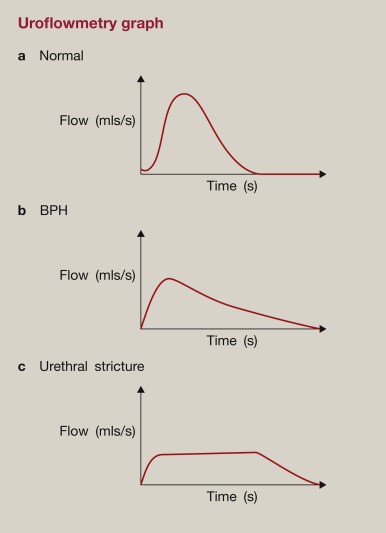
Uroflowmentry: Flow profile of a patient is often enough to clench the diagnosis. The graph from a stricture urethra patient has an extended urination time with a low-level plateau .The shape of this curve is pathognomonic of urethral stricture disease.
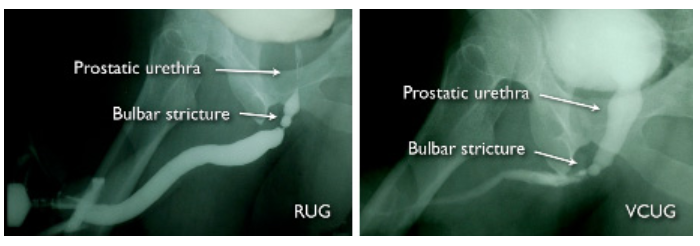
Retrograde Urethrogram and Voiding Cystourethrogram (RUG/VCUG): These are special dye radiograms (X-Rays) to determine the site and length of stricture.
Urethroscopy: Though required rarely, but may be helpful to diagnose stricture disease in unsuspected patients.
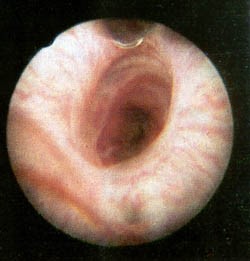
Bulbar Urethral Stricture on Urethroscopy
If the patient presents with retention of urine or dilatation of the upper urinary tracts, the first step in the management is urinary diversion, usually by supra-pubic cystostomy. Definitive surgical procedure is done after management of urinary tract infection and correction of the hemodynamic and renal function parameters.
Surgical management of the urethral stricture disease can be endourological or open reconstructive surgery.
Endourological Management (Optical Internal Urethrotomy)- in this procedure the stricture scar is incised endoscopically using cold steel knife/ laser to obtain a widened urethral tube. The expanded wound margins heal with secondary intention. However there is a high chance of recurrence with this procedure, and thus it is now used only for first time short segment bulbar urethral strictures (<2cm).
Open Reconstructive Surgery (Urethroplasty)- Mainstay treatment of the urethral stricture disease. Various forms of reconstructive surgeries are employed depending on the length of the stricture disease, site of stricture and patient characteristics. These include-