UROLITHIASIS OR NEPHROLITHIASIS (URINARY TRACT STONES)
Urinary tract stones affect approximately 1 in 11 people (19 percent of men and 9 percent of women by age 70 years). Fortunately, treatment is available to effectively manage them and steps can be taken to prevent their recurrence.
Aetiology of urolithiasis is usually multifactorial. The most common reason may be urine that is supersaturated with salt and minerals such as calcium oxalate, struvite (ammonium magnesium phosphate), uric acid and cystine. This may occur due to dehydration (low water content in body) or an excess secretion of these solutes by the kidney. Certain risk factors are also known to enhance the susceptibility of a persons urinary tract to form stones. These include anatomical abnormalities or obstruction of the urinary tract, gout, hyper-parathyroidism , genetic predisposition or consumption of certain group of drugs( e.g diurteics, topiramate etc).
PRESENTATION
Most common symptoms of stone disease include-
Pain (classically starting from loin and radiating to the lower abdomen or groin)
Hematuria (blood in urine)
Fever with chills.
Dysuria (burning in urine)
Obstructive urinary flow
However in many patients these stones are detected incidentally on investigations done for other reasons.
Though the investigation protocol varies from patient to patient, the common tests employed are-
Urine examination to look for Red Blood Cell, Pus cells etc
Blood examination to assess Kidney Function
Ultrasound Examination
Intravenous Urography
Non Contrast C.T KUB
T. IVP
DTPA renal scan to assess kidney function in poor functioning kidneys.
INVESTIGATIONS
MEDICAL MANAGEMENT
Medical management can be offered to most patients with adequate renal function when the stones are small (<7mm) and thus have a high probability of spontaneous passage on medical expulsion therapy. The main components of medical expulsion therapy include rehydration, pain relief and medicines aimed at relaxing the urinary passage for easy migration of the calculi. This can be continued for a period of 3-4 wks. However in the event of failure of spontaneous passage or development of complications as infection or worsening of renal function patient is advised to progress for surgical management.
Medical expulsion therapy is not advisable for patients with solitary kidney, bilateral hydroureteronephrosis, renal failure or anuria.
SURGICAL MANAGEMENT
Surgical intervention is usually required in 20% of all cases with urolithiasis and in most patients with stones >8mm in diameter.
PROCEDURES TO REMOVE STONES INCLUDE
Extracorporeal shock wave lithotripsy (ESWL) – A day care procedure wherein shock waves from a generator are focussed on the stone. Stone particles generated pass spontaneously with urine. Reserved for cases with renal and upper ureteric stones (<20mm) without gross dilatation of the urinary tract and a good renal function. The procedure may take more than one sitting (usually done at an interval of 7-10days).
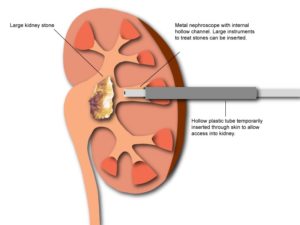
Percutaneous nephrolithotomy (PCNL) – Keyhole endoscopic surgery done under anesthesia for large (>20mm)stones. A small endoscopic instrument (nephroscope) is passed through the skin (percutaneously) from back into the kidney. Stones are fragmented using Laser or Pneumatic Lithoclast and subsequently removed.
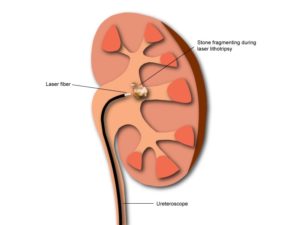
Ureteroscopy (URS)/Retrograde Intrarenal Surgery (RIRS) – A thin endoscopic instrument is passed from the lower urinary tract to ureter or kidney and stone is fragmented using Laser. This has excellent results in the hands of experts.
Laparoscopic /Open surgery – rarely necessary and usually reserved for complicated cases (anatomical abnormalities , failed endoscopic surgeries etc)
PREVENTION
Stone analysis and metabolic evaluation should be carried out in all cases with recurrent urolithiasis, paediatric urolithiasis and in patients with urolithiasis in solitary kidney.
Urolithiasis is a disease with recurrent nature. Thus regular follow up and modifications in diet and lifestyle are needed.
COMMON MODIFICATIONS INCLUDE
Increase fluid intake (3 litres/day). Patient is encouraged use of lemon water, pineapple or cranberry juice as these contain inhibitors of stone formation.
Reduce intake of salts and animal proteins.
Depending on the composition of stone specific dietary modifications can be advised.
Certain medicines can be prescribed for long term use depending on the type of stone.